Twijfels over cardioprotectief effect β-blokkers
16/10/2012
Bètablokkers verbeteren uitkomsten bij patiënten met CAD waarschijnlijk niet. (met slides).
β-Blocker use and clinical outcomes in stable outpatients with and without coronary artery disease.Literatuur - Bangalore S. et al. REACH Registry Investigators - JAMA. 2012;308:1340-9
Bangalore S, Steg G, Deedwania P, et al; REACH Registry Investigators.
JAMA. 2012;308:1340-9. doi: 10.1001/jama.2012.12559.
Achtergrond
Voor patiënten met coronaire hartziekten (CAD) blijven β-blokkers de standaard van zorg, vooral na een myocardinfarct (MI) [1,2]. De gegevens uit post-MI of hartfalen trials zijn geëxtrapoleerd naar patiënten met CAD of een hoog risico op CAD. Het is niet duidelijk of het gebruik van beta-blokkers zal leiden tot een lager risico van samengestelde CV gebeurtenissen bij patiënten met risicofactoren voor CAD alleen, een bekend eerder MI of bekende CAD zonder MI. Een longitudinale, observationele studie in patiënten in de Reduction of Atherothrombosis for Continued Health (REACH) registry werd daarom uitgevoerd. Patiënten werden verdeeld in drie cohorten: bekend eerder MI (n = 14.043) bekende CAD zonder MI (n = 12.012) of met CAD risicofactoren alleen (n = 18.653). Primaire uitkomstmaat werden gedefinieerd als een samenstelling van CV overlijden, niet-fataal MI of niet-fataal CVA, en de secundaire uitkomst als de primaire uitkomstmaat plus ziekenhuisopname voor atherotrombotische complicaties of een revascularisatie procedure.
Belangrijkste resultaten
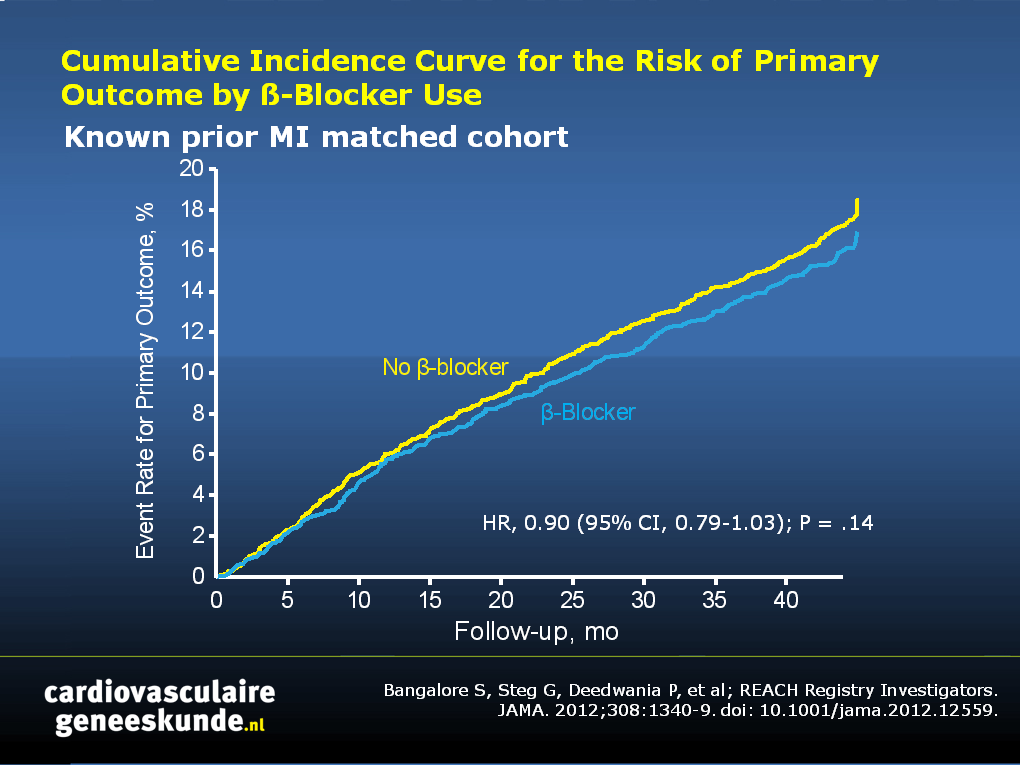
Bètablokkergebruik was niet geassocieerd met een significant verschil in het optreden van cardiovasculaire sterfte, niet-fataal MI of niet-fataal CVA:CAD patiënten met eerder MI:
- 16,93% in de bètablokker groep versus 18,60% in de controlegroep, hazard ratio [HR] 0,90, CI 0,79-1,03, p = 0,14
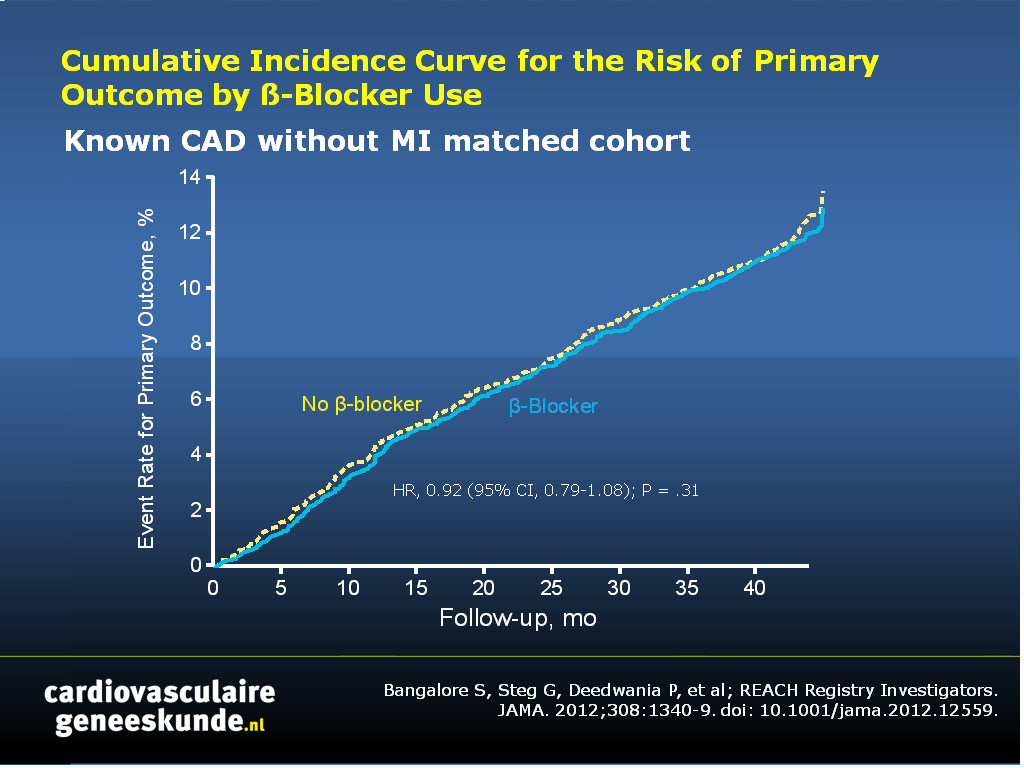
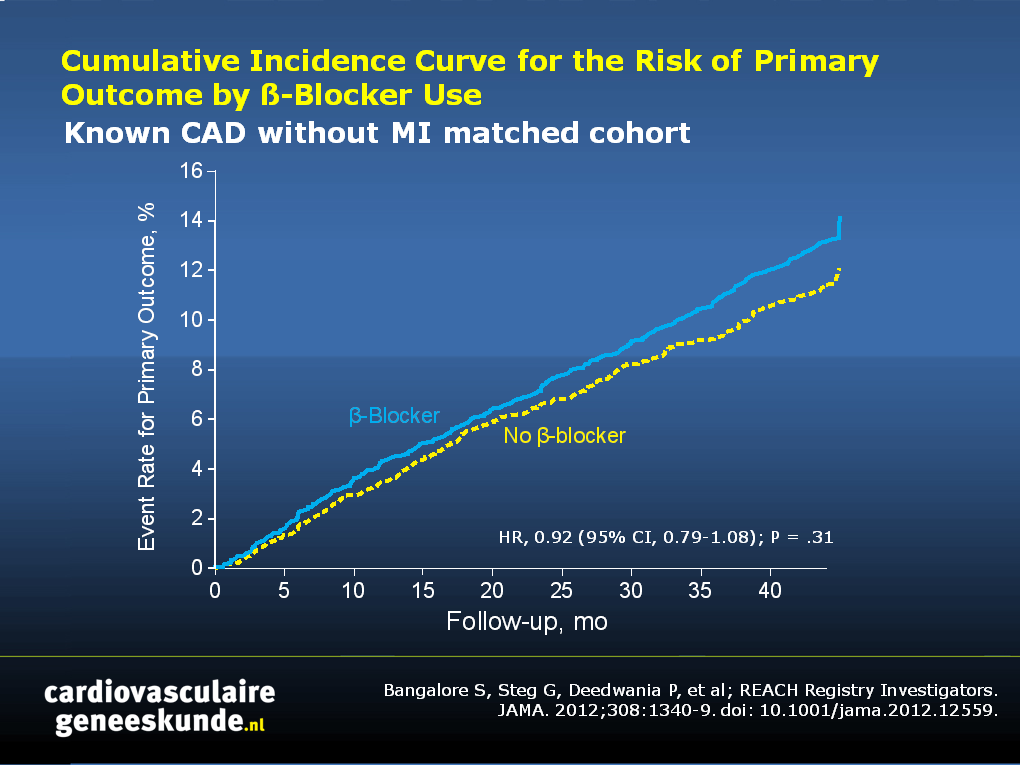
CAD patiënten zonder voorafgaande MI:
- 12,94% versus 13,55%, HR 0,92, BI 0,79-1.08, p = 0,31
Patiënten met alleen risicofactoren:
- 14,22% versus 12,11%, HR 1,18, CI 1.02-1,36, p = 0,02
Conclusie
β-Blokkergebruik was niet geassocieerd met een lagere incidentie van cardiovasculaire gebeurtenissen bij 44 maanden follow-up, zelfs bij patiënten met een voorgeschiedenis van MI, hetgeen in overeenstemming is met de recent bijgewerkte American Heart Association secundaire preventie richtlijnen waarin bètablokker therapie een klasse I aanbeveling is alleen voor HF, MI of ACS tot 3 jaar na MI, maar een klasse IIa aanbeveling is voor de langere-termijn therapie. Verder onderzoek is nodig om subgroepen te identificeren die profiteren van β-blokker behandeling en de optimale duur van β-blokker therapie.Fig. 1-3. Cumulatieve incidentiecurve voor het risico van primaire uitkomst naar β-blokker gebruik
Download Bangalore S jama 2012.pptx
Referenties
Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357:1385-1390.Chen J, Radford MJ, Wang Y, et al. Are β-blockers effective in elderly patients who undergo coronary revascularization after acute myocardial infarction? Arch Intern Med. 2000; 160:947-952.
Abstract
Context:
β-Blockers remain the standard of care after a myocardial infarction (MI). However, the benefit of β-blocker use in patients with coronary artery disease (CAD) but no history of MI, those with a remote history of MI, and those with only risk factors for CAD is unclear.
Objective:
To assess the association of β-blocker use with cardiovascular events in stable patients with a prior history of MI, in those with CAD but no history of MI, and in those with only risk factors for CAD.
Design, setting, and patients:
Longitudinal, observational study of patients in the Reduction of Atherothrombosis for Continued Health (REACH) registry who were divided into 3 cohorts: known prior MI (n = 14,043), known CAD without MI (n = 12,012), or those with CAD risk factors only (n = 18,653). Propensity score matching was used for the primary analyses. The last follow-up data collection was April 2009.
Main outcome measures:
The primary outcome was a composite of cardiovascular death, nonfatal MI, or nonfatal stroke. The secondary outcome was the primary outcome plus hospitalization for atherothrombotic events or a revascularization procedure.
Results:
Among the 44,708 patients, 21,860 were included in the propensity score-matched analysis. With a median follow-up of 44 months (interquartile range, 35-45 months), event rates were not significantly different in patients with β-blocker use compared with those without β-blocker use for any of the outcomes tested, even in the prior MI cohort (489 [16.93%] vs 532 [18.60%], respectively; hazard ratio [HR], 0.90 [95% CI, 0.79-1.03]; P = .14). In the CAD without MI cohort, the associated event rates were not significantly different in those with β-blocker use for the primary outcome (391 [12.94%]) vs without β-blocker use (405 [13.55%]) (HR, 0.92 [95% CI, 0.79-1.08]; P = .31), with higher rates for the secondary outcome (1101 [30.59%] vs 1002 [27.84%]; odds ratio [OR], 1.14 [95% CI, 1.03-1.27]; P = .01) and for the tertiary outcome of hospitalization (870 [24.17%] vs 773 [21.48%]; OR, 1.17 [95% CI, 1.04-1.30]; P = .01). In the cohort with CAD risk factors only, the event rates were higher for the primary outcome with β-blocker use (467 [14.22%]) vs without β-blocker use (403 [12.11%]) (HR, 1.18 [95% CI, 1.02-1.36]; P = .02), for the secondary outcome (870 [22.01%] vs 797 [20.17%]; OR, 1.12 [95% CI, 1.00-1.24]; P = .04) but not for the tertiary outcomes of MI (89 [2.82%] vs 68 [2.00%]; HR, 1.36 [95% CI, 0.97-1.90]; P = .08) and stroke (210 [6.55%] vs 168 [5.12%]; HR, 1.22 [95% CI, 0.99-1.52]; P = .06). However, in those with recent MI (≤1 year), β-blocker use was associated with a lower incidence of the secondary outcome (OR, 0.77 [95% CI, 0.64-0.92]).
Conclusion:
In this observational study of patients with either CAD risk factors only, known prior MI, or known CAD without MI, the use of β-blockers was not associated with a lower risk of composite cardiovascular events.